In 1976, a chemist named Alexander Shulgin synthesized a molecule that had been sitting in a patent filing since 1912 and decided to try it himself. What he experienced over the next several hours would eventually reshape psychiatric medicine.
In this article
The compound was 3,4-methylenedioxymethamphetamine. Shulgin called it by the shorthand MDMA. He described the experience in his notes as producing "an easy warmth, a feeling of being comfortable with yourself and with others." Over the following years, he shared it with dozens of therapists who quietly began using it with patients — believing they had found something genuinely new: a drug that made people feel safe enough to confront their worst memories without being overwhelmed by them.
That experiment in underground therapy was shut down in 1985, when the Drug Enforcement Administration placed MDMA in Schedule I. But the research thread never fully broke. Today, after decades of persistence by a small advocacy organization called MAPS and hundreds of millions of dollars in clinical trials, MDMA sits at the center of the most significant development in trauma treatment in a generation.
What Is MDMA? Chemistry, Names, and Mechanism
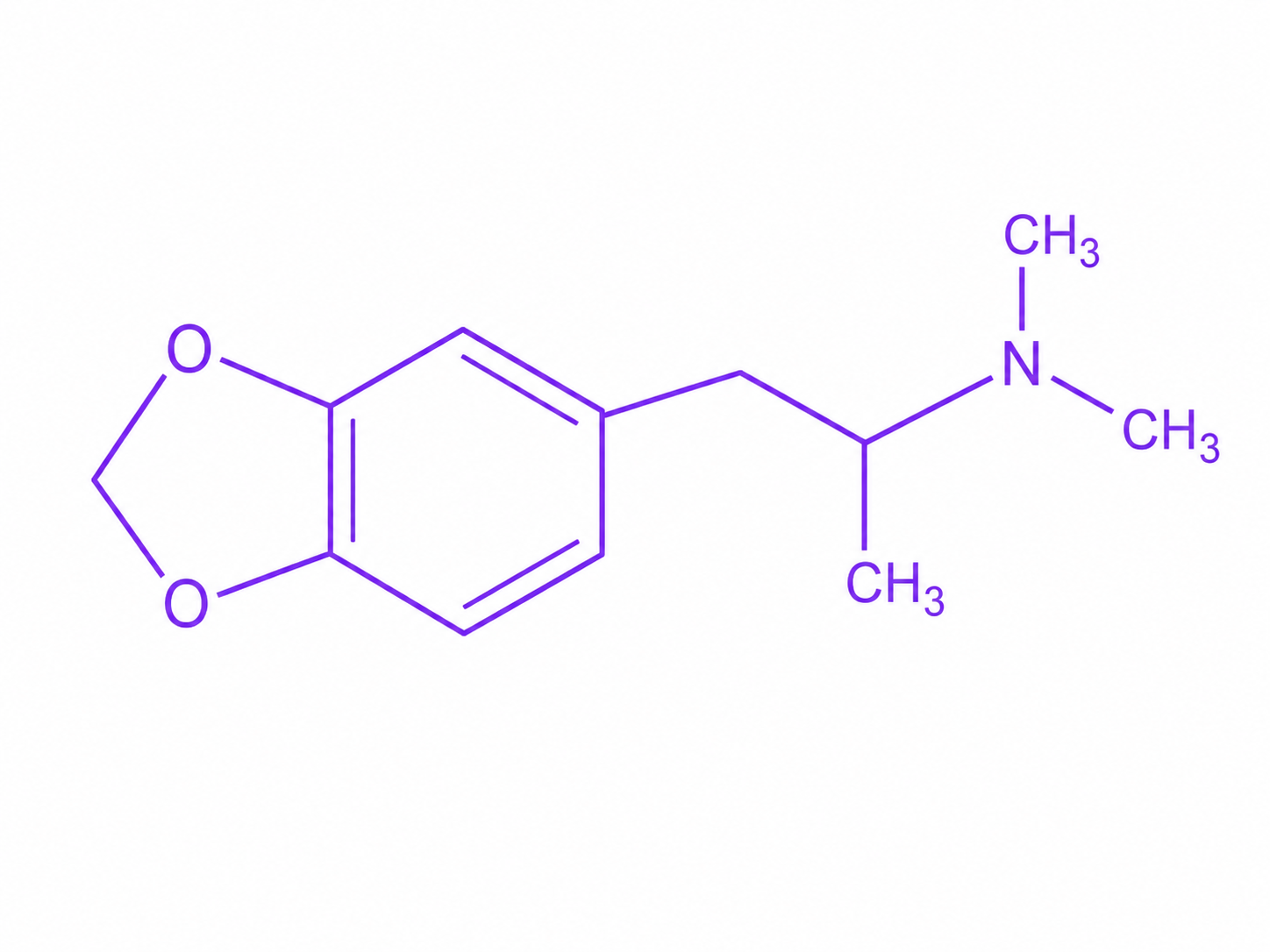
MDMA belongs to the phenethylamine and amphetamine chemical families. Its full name, 3,4-methylenedioxymethamphetamine, describes its structure: a methamphetamine backbone with a methylenedioxy ring substitution that dramatically changes how it behaves in the body.
It goes by many names. Ecstasy refers to pressed tablets sold on the illicit market, which frequently contain adulterants or substitutes. Molly refers to powder or crystal form, marketed as purer MDMA, though testing consistently finds impurities in street samples as well. In clinical trials, researchers use pharmaceutical-grade MDMA synthesized to known purity and dosage.
MDMA's mechanism of action is more complex than most psychoactive drugs. It is a potent releaser of three monoamine neurotransmitters: serotonin, dopamine, and norepinephrine. It forces these transmitters out of storage vesicles and into the synapse, producing a massive flood. It also inhibits their reuptake transporters, preventing the synapse from clearing them quickly.
The serotonin surge dominates the pharmacological picture. MDMA releases approximately three times as much serotonin as dopamine, which distinguishes it from classical stimulants like cocaine or amphetamine, where dopamine is the primary driver. This ratio explains much of what makes MDMA feel different: less jittery euphoria, more emotional openness and warmth.
MDMA also triggers the release of oxytocin from the hypothalamus, a neuropeptide associated with social bonding and trust. Studies measuring blood oxytocin levels after MDMA administration show significant increases. Researchers at Imperial College London have linked this oxytocin release to MDMA's prosocial effects — the feeling of closeness to others, reduced defensiveness, and increased empathy that users consistently report and that therapists in the 1980s found clinically valuable.
The Shulgin and MAPS Origin Story
Merck first synthesized MDMA in 1912 as part of a patent for a blood-clotting compound. The company never developed it, and it sat largely unexamined in the chemical literature for sixty years.
Shulgin's 1976 synthesis changed that. He was a consultant pharmacologist with an unusual combination of credentials and curiosity: a doctorate in biochemistry from UC Berkeley, professional connections to the DEA that gave him a Schedule I researcher license, and a personal commitment to exploring the phenomenology of psychoactive compounds. His lab notebooks from this period, later published in the book PiHKAL, describe hundreds of self-experiments conducted with methodical precision.
Shulgin introduced MDMA to a psychotherapist named Leo Zeff, who became an early champion. Zeff trained dozens of therapists in its use, and by the early 1980s, an estimated half million doses had been administered in underground therapeutic contexts. Therapists using it reported that patients were able to discuss traumatic events with unusual clarity and emotional stability — accessing painful material without the avoidance and hyperarousal that typically made such work difficult or impossible.
The DEA's 1985 emergency scheduling of MDMA shut that experiment down. But it simultaneously catalyzed organized resistance. Rick Doblin, then a graduate student, founded MAPS in 1986 with the explicit goal of winning FDA approval for MDMA-assisted therapy. The path would take four decades.
MDMA-Assisted Therapy: MAPS Phase 3 Trials
MAPS spent the 1990s and 2000s navigating a slow regulatory obstacle course: establishing safety data, winning approval for Phase 1 studies, then Phase 2. The Phase 2 trials, completed across multiple sites between 2004 and 2017, showed promising results for PTSD. In a pooled analysis of six trials, 54 percent of participants receiving MDMA-assisted therapy no longer met diagnostic criteria for PTSD at the primary endpoint, compared to 23 percent in placebo-controlled therapy.
In 2017, the FDA granted MDMA a Breakthrough Therapy designation for PTSD — an expedited development pathway for drugs treating serious conditions where preliminary evidence shows substantial improvement over existing therapies. The designation reflected the agency's assessment that PTSD treatment outcomes with available medications and psychotherapy are genuinely inadequate: roughly half of patients with PTSD do not respond to first-line treatments, and those who do often retain significant residual symptoms.
MAPS launched Phase 3 trials in 2018 across 15 sites in the US, Canada, and Israel. The study enrolled 90 participants, all with severe PTSD, who were randomized to receive three sessions of MDMA-assisted therapy (80 or 120 mg dose, with optional 40 or 60 mg supplemental dose) or three sessions of placebo-assisted therapy. Both groups received the same manualized therapy protocol before, during, and after each session.
Results published in Nature Medicine in 2021 showed that 67 percent of participants in the MDMA group no longer met PTSD diagnostic criteria at the primary endpoint, compared to 32 percent of placebo participants. Functional impairment scores showed similar separation. A second Phase 3 trial completed in 2022 replicated the findings, with 71 percent of MDMA recipients no longer meeting PTSD criteria versus 48 percent in the placebo group.
The 2024 FDA Rejection and What Comes Next
In August 2024, the FDA declined to approve MDMA-assisted therapy for PTSD, issuing a Complete Response Letter that cited several concerns. The agency's advisory committee had voted 9-2 that the available data failed to demonstrate effectiveness, and 10-1 that the benefits did not outweigh the risks — a striking rebuke for a drug that had been given Breakthrough Therapy designation seven years earlier.
The committee's concerns were specific. Blinding was imperfect: most participants could tell whether they had received MDMA or placebo, creating potential for expectancy bias to inflate outcomes. The agency wanted a functional unblinding analysis and additional data on the durability of effects. It also raised questions about trial conduct, including concerns about protocol deviations at specific sites that were flagged during a clinical inspection.
Lykos Therapeutics, the for-profit subsidiary MAPS spun out to run the regulatory submission, indicated it would work with the FDA to address the deficiencies. The agency requested an additional Phase 3 trial, which as of 2025 is being designed. The timeline for any eventual approval has been pushed back to the late 2020s at the earliest.
Enjoying this? Subscribe free.
Twice a week: psychedelic science, policy, and culture, decoded for humans.
You'll also get our free Top 10 Psychedelic Books guide.
You're in! Redirecting to your free guide...
The rejection was a significant setback, but it did not end the research program. MDMA-assisted therapy remains legal within clinical trials. Expanded access programs allow patients who don't qualify for trials to receive the treatment through a separate regulatory pathway. And the scientific interest generated by the MAPS trials has drawn new investigators and funders into the field, broadening the research base beyond any single organization.
What the Research Shows
PTSD is the primary indication that has driven MDMA research, but the literature extends into adjacent areas.
A small open-label study published in 2021 examined MDMA-assisted therapy for alcohol use disorder, finding significant reductions in drinking days and alcohol use severity at nine months follow-up. The sample was too small for definitive conclusions, but the signal was strong enough to justify controlled trials.
Research into MDMA for couples therapy, conducted by researchers at UCSF and published in 2022, found that MDMA administered to both partners simultaneously produced significant improvements in relationship satisfaction and dyadic adjustment at the six-month follow-up. This approach, which has no direct analog in mainstream psychiatry, has drawn interest from researchers studying relationship distress as both a standalone problem and a driver of individual mental health outcomes.
Social anxiety in autistic adults has been another focus. A Phase 2 trial at Stanford found MDMA-assisted therapy produced significant reductions in social anxiety symptoms in autistic adults, with effects persisting at six months. The rationale draws directly on MDMA's oxytocin-mediated prosocial effects: for individuals whose social anxiety is rooted in fear of judgment or rejection, a drug that temporarily suspends that fear may allow new experiences of social connection to form.
Eating disorders, treatment-resistant depression, and end-of-life anxiety are among the other conditions being explored. The research base is still early in most of these areas, but the consistency of findings across indications involving trauma, fear, and avoidance has researchers paying attention to a shared underlying mechanism.
Effects and Risks
Acutely, MDMA produces feelings of emotional warmth, increased empathy, reduced fear and defensiveness, heightened sensory perception, and mild stimulation. The subjective experience typically lasts three to five hours, with a longer tail of more subtle effects. Most users report feeling reflective and calm in the days following an experience, though some report a period of low mood — often called a "comedown" — in the days after, attributed to temporary depletion of serotonin stores.
The neurotoxicity debate has been a persistent feature of MDMA research since the late 1980s. Animal studies using high, repeated doses showed evidence of serotonergic axon terminal damage in rats and primates. Human neuroimaging studies have found differences in serotonin transporter density in heavy ecstasy users, though the interpretation of these findings is complicated by the difficulty of isolating MDMA from other substances in polydrug user populations, and by confounds like pre-existing differences between users and non-users.
Researchers at Johns Hopkins and elsewhere have noted that the doses used in clinical trials (typically 80-120 mg, given two to three times over several months) are dramatically lower than the doses used in most neurotoxicity studies, and that rest periods between doses allow serotonin systems to recover. The Phase 3 PTSD trials showed no evidence of serotonergic damage on neuropsychological testing or imaging.
Serotonin syndrome is a serious risk when MDMA is combined with other serotonergic drugs, particularly monoamine oxidase inhibitors (MAOIs), SSRIs, or other serotonin releasers. The condition can be life-threatening. This is why MDMA-assisted therapy protocols require washout periods from psychiatric medications before dosing sessions, and why harm reduction organizations emphasize drug interaction checking as a first priority for anyone using MDMA outside clinical settings.
Cardiovascular effects are real: MDMA raises heart rate and blood pressure during the acute period. People with pre-existing cardiac conditions, uncontrolled hypertension, or certain arrhythmias face elevated risk. Clinical trial screening protocols exclude these patients.
Hyperthermia and hyponatremia are the two mechanisms behind most MDMA-related deaths in recreational contexts. Hyperthermia occurs when people dance intensely for long periods in hot environments without adequate cooling; MDMA's heat-regulation effects compound the problem. Hyponatremia occurs when people overcorrect by drinking excessive water, diluting blood sodium to dangerous levels. Basic harm reduction guidance addresses both: take breaks, maintain moderate fluid intake, and avoid mixing with stimulants or alcohol.
Legal Status and Policy Landscape
MDMA is Schedule I under federal law, classified as having high abuse potential and no accepted medical use. This classification predates any of the modern clinical research and is under active challenge from researchers who argue that the scheduling criteria have not kept pace with the evidence.
At the state level, movement has been slower than with psilocybin. Colorado's Proposition 122, passed in 2022, included MDMA in its natural medicine framework — but only for psilocybin and psilocin in the initial regulatory rollout, with MDMA subject to further review. No state has yet created a licensed treatment framework specifically for MDMA.
Australia moved faster than the United States. In February 2023, the Therapeutic Goods Administration approved MDMA for use in MDMA-assisted therapy for PTSD through authorized prescribers — the first country in the world to do so. The program launched in July 2023, with registered psychiatrists able to prescribe pharmaceutical-grade MDMA to eligible PTSD patients.
Canada, Israel, and several European countries have active research programs, and compassionate access pathways allow some patients to receive the treatment outside of trials. The international divergence from US federal policy mirrors the earlier trajectory of cannabis legalization and is watched closely by domestic advocates.
For a state-by-state look at where psychedelic laws currently stand in the US, see the US Psychedelic Laws Map.
The Future of MDMA Therapy
The path to FDA approval is longer than it appeared in 2021, but the scientific case has not weakened. The 2024 rejection was primarily procedural and methodological, not a finding that MDMA-assisted therapy doesn't work. The advisory committee's concern about blinding is real but not fatal: drug trials for conditions with obvious subjective effects routinely face this challenge, and researchers are developing expectancy-adjusted analysis methods to address it.
The population that stands to benefit is large. An estimated 13 million Americans currently have PTSD. Military veterans, survivors of sexual assault, first responders, and refugees are among the groups with the highest prevalence and the poorest outcomes with existing treatments. The inadequacy of current options is not a point of controversy in psychiatry.
New investigators outside of MAPS are now running MDMA trials, which matters for the regulatory process: independent replication is exactly what the FDA is asking for. The NIMH has funded MDMA research. Academic centers including Johns Hopkins, Yale, NYU, and UCSF have active programs. The institutional infrastructure that psychedelic research lacked twenty years ago now exists.
Shulgin died in 2014, before the Phase 3 results were published. Rick Doblin stepped down from MAPS leadership in 2024. The movement he built is now larger than any single organization, and the question is no longer whether MDMA will eventually enter medicine but when, in what form, and for whom.
That question is being answered in real time. Understand the full landscape with the US Psychedelic Laws Map, or explore the science of related compounds like psilocybin and microdosing.
Enjoying this? Subscribe free.
Twice a week: psychedelic science, policy, and culture, decoded for humans.
You'll also get our free Top 10 Psychedelic Books guide.
You're in.
Redirecting to your free book guide...